
Anterior Delormes Procedure for the treatment of Rectocele
What is an Anterior Delormes?
This is an operation performed via your back passage (anus) to repair the rectocele.
What is a rectocele?
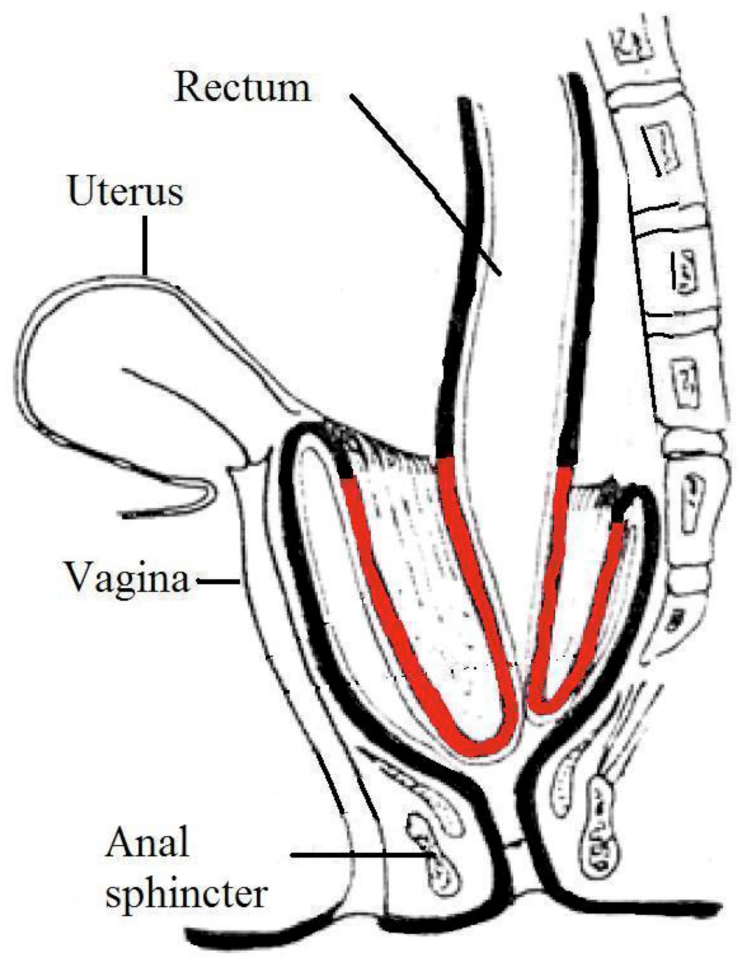
A rectocele is a bulge of the lower rectum into the back of the vagina due to a weakness in the tissues. This may be a result of child birth or repeated straining when opening your bowels. It is also commonly found in people without symptoms. Symptoms may include:
- The feeling of a lump in your vagina and difficulty evacuating faeces with this sensation
- The feeling that you are not emptying your bowels completely
- You may leak faeces into your underwear without knowing
- You may need to place your finger into your rectum or apply pressure against your perineum to help empty your bowels.
Reasons for having an Anterior Delormes.
Many people have this condition and do not have many symptoms; however, if your symptoms have not improved with pelvic floor physiotherapy and are particularly bothersome then an Anterior Delormes Procedure may help relieve these.
Alternative treatments
You may choose not to have surgery as your symptoms are manageable or you may wish to continue with your pelvic floor physiotherapy. If your rectocele is very large then you may need to have a different operation that a member of your surgical team will discuss with you in clinic.
Diagnosis
Before your surgeon decides to do this operation, you will have had several tests performed to assess your bowel properly.
- Endoscopy to look at the inside of your bowel (a Flexible sigmoidoscopy, or a Colonoscopy),
- Anorectal physiology and ultrasound to take some measurements of your sphincter muscles
- Proctogram - an X ray to show your bowel and pelvic muscles working, and to see how well supported your pelvic organs are.
- Physiotherapy - You will have been given pelvic floor exercises to complete.
You would have also dietary and bowel management advice before surgery is decided. This will all be useful for your recovery.
What does the procedure involve?
All the surgery is done through your back passage (anus) and therefore there are no stitches on the outside. The bowel lining on top of the bulge (rectocele) is stripped off and the muscle wall is stitiched together to strengthen the wall between bowel and vagina. This is usually completed as a day surgery.
What about the anaesthetic?
This surgery will be performed under general anaesthetic, you will be seen by your anaesthetist on the day of your surgery to discuss the anaesthetic in more detail.
What happens before the operation?
Prior to your admission you will have seen a member of the surgical team to discuss the surgery and its risks and benefits.
You will have a pre-operative assessment where you are likely to be examined by a practitioner, have bloods taken and be asked about your past medical history, previous surgeries and asked about any medications you may be taken. At times you may be asked to stop taking certain medications prior to surgery, these may impose an added risk to surgery such as blood thinning medications.
You will receive a letter detailing the date of your surgery, time and ward to report to for your admission. You will also be advised on what to bring to hospital with you.
Upon admission on to the ward you will be shown where to sit, where you will be see a number of different people. You will be seen by a nurse who will take some information from you and will attach patient identification bands around your wrists or ankles. You will be given a gown to wear for theatre and white stockings to wear to help prevent blood clots. You will also be seen by a member of the surgical team who will go through the consent form for your procedure with you, an anaesthetist who will discuss your anaesthetic. You will also be given an enema to empty your bowel prior to surgery. Please stay on the ward so that you may be seen by all these people to avoid delays in your surgery.
When your theatre team is ready for you, a member of the theatre team will come to the ward to collect you; they will check a few details with you and then walk you to theatre if you are able. You will be taken into the anaesthetic room where you will be met by your anaesthetist. A member of the theatre team will ask you to lie on a theatre bed, and will attach a blood pressure cuff to your arm; a probe onto your finger to measure your oxygen levels and three round stickers attached to wires will be placed onto your chest to monitor your heart. You will also have a need placed into a vein on the back of your hand or arm; this allows the anaesthetist to administer the medications required for your anaesthetic.
What happens after the operation?
When you are awake and feel ready you will be given something to eat and drink. You will be encouraged to get up and use the toilet. When you are comfortable you will be allowed to go home (this is generally later that same day). Please make sure you have somebody to collect you as you will not be able to drive. You must also ensure that you have somebody to stay with you for 24 hours following your surgery whilst you are recovering from your anaesthetic.
You will be prescribed stool softeners as it is very important that you do not get constipated and strain to open your bowels as this would affect the success of the operation. You may find that you are slightly sore following your operation but simple pain killers such as paracetamol should help with this.
If your surgeon has placed an absorbent dressing into your bottom during surgery (your surgeon will advise you of this), you will pass this next time you open your bowels.
You can shower and bath after the operation and this is helpful in keeping the area as clean as possible. You may return to driving again 2-3 days after surgery when you feel you are able to complete an emergency stop, return to work after 2 weeks but should not do any lifting for at least 6 weeks.
We expect you to make a rapid recovery after your operation and to experience no serious problems. However, it is important that you should know about minor problems, which are common after this operation, and also about more serious problems that can occasionally occur.
What problems can occur after the operation?
Bleeding – you may experience a small of bleeding from your bottom, this is more likely if you are taking blood thinning medications.
Infection – although relatively uncommon, due to the site of operation you are at risk of developing an infection, this is usually treated effective with antibiotics.
Abscess formation – it is possible, although uncommon to develop an abscess, treatment for this would include antibiotics and/or surgery.
Recto-vaginal Fistula – this is when an abnormal connection between your rectum and fistula forms, allowing gas and stool to be passed through your vagina. This will need to be corrected by surgery.
Deep vein thrombosis (DVT) - is a possible problem, but is uncommon. If you are at particular risk then special precautions will be taken to reduce the risk. Moving your legs and feet as soon as you can after the operation and walking about early, all help to stop thrombosis occurring.
Failure to resolve symptoms – there is always a chance that this surgery will not resolve your symptoms, if this is the case then your surgeon will discuss further options with you in clinic.
The risks of a general anaesthetic
General anaesthetics have some risks, which may be increased if you have chronic medical conditions, but in general they are as follows:
- Common temporary side effects (risk of 1 in 10 to 1 in 100) include bruising or pain in the area of injections, blurred vision and sickness, these can usually be treated and pass off quickly.
- Infrequent complications (risk of 1 in 100 to 1 in 10,000) include temporary breathing difficulties, muscle pains, headaches, damage to teeth, lip or tongue, sore throat and temporary problems with speaking.
- Extremely rare and serious complications (risk of less than 1 in 10,000). These include severe allergic reactions and death, brain damage, kidney and liver failure, lung damage, permanent nerve or blood vessel damage, eye injury, and damage to the voice box. These are very rare and may depend on whether you have other serious medical conditions.
What should you do if you develop problems?
In the first incidence you should contact your GP, your GP will then decide on the most appropriate treatment for you, and will be able to contact your surgeon if necessary.
Do you need to return to hospital for a check?
You will be sent an appointment to attend an outpatients clinic; this will usually be in 6-8 weeks following surgery.
Who should you contact in an emergency?
In the event of an emergency attend your local accident and emergency department, however, if your condition is life threatening call for an ambulance.
Book a consultation with Miss Boorman today.
Laparoscopic Ventral Rectopexy
A ’rectopexy’ is an operation to fix the rectum back into its normal anatomical position.
One of the common reasons for this operation is for full thickness external rectal prolapse or internal prolapsing (‘intussusception’) of the rectal wall, causing difficulty in emptying the bowel. The bowel wall collapses in on itself during straining, and can cause a sense of blockage, difficulty in passing a motion, a need for prolonged, sometimes unsuccessful attempts to empty the bowel (Obstructed Defecation Syndrome – ODS). Sometimes there is a need to support or apply pressure to the perineum to help, or insert a finger into the vagina or rectum to empty the bowel. The rectal prolapse can sometimes cause some faecal incontinence as well, and a ventral rectopexy may improve these symptoms.

This operation is done laparoscopically (keyhole) under general anaesthetic, and takes about 1½ hours. There will be a small cut below your umbilicus (tummy button) and 2 other small cuts on your right side.
Inside the abdomen, the uterus is lifted forward, and a pocket is dissected between the front of the rectum and the vagina into which a piece of mesh is inserted, and stitched into place. The top end is fixed to the sacrum (end of the back bone). This mesh then splints the rectum into its proper position, lifting it up out of the pelvis, and prevents it telescoping in on itself and prolapsing as before. The vagina may be stitched to the mesh to prevent a vaginal prolapse, and any rectocoele (bulge of the rectum into the vagina) or enterocoele (bulge of bowel from higher up dropping into the pelvis between rectum and vagina).

Before Surgery
Before your surgeon decides to do this operation, you will need to have several tests so that your bowel can be properly assessed: You will need an endoscopy to look at the inside of your bowel (a Flexible sigmoidoscopy, or a Colonoscopy), some measurements of your sphincter muscles (anorectal physiology and ultrasound), and an X ray to show your bowel and pelvic muscles working, and to see how well supported your pelvic organs are (proctogram). You will probably be given pelvic floor exercises, dietary and bowel management advice before surgery is decided. This will all be useful for your recovery.
While you are waiting for your operation, try and prepare yourself physically. Try and eat a healthy well-balanced diet including meat (unless vegetarian), fresh fruit and vegetables, and plenty of fluid ie 8-10 cups daily.
Take exercise such as walking, swimming etc. If you smoke, we strongly advise you to stop.
You will see a Pre-assessment nurse before your operation, for a health check. If you are taking any medication please bring them all with you. Your blood pressure will be checked, and you may have an ECG (heart trace) and a chest X-ray. You will also have blood taken. This information is all needed by the anaesthetist for planning your anaesthetic.
The Pre-assessment nurse will explain the admission process to you so that you know what to expect, and answer any questions you may have. If you live alone and have no friends or family to help you, please let us know, and we will try and organise necessary arrangements.
You will usually be admitted to the ward on the morning of your operation. As with any surgery, you will need to stop eating 6 hours before surgery, though you may drink clear, still fluids until 2hours before. You will be given an enema to empty your bowel before your operation. Your anaesthetist will see you before your operation, and the surgeon will also ask you to sign your consent form, and give you an opportunity to ask any further questions.
You will also be given stockings to wear, and a blood thinning injection, to help prevent blood clots forming. You will be asked to change into a theatre gown, so that you are ready for the Theatre staff to walk with you to Theatre. Your details will be checked at regular stages during the process.
Risks of Surgery
Every operation carries a risk – this can be increased by pre-existing health conditions and general poor fitness of the patient. This is relatively low risk surgery because bowel is not removed and the nerves to the rectum and genitalia are avoided.
Occasionally there can be recurrence for people who have repair of an external prolapse, but this is less than 2%, and rarely, people may experience no improvement following surgery, though for those with ODS, the majority experience a significant improvement, as do those with incontinence due to internal prolapse. Occasionally, if you have had extensive abdominal surgery , you may not be suitable for laparoscopic surgery.
Most people will not experience any serious complications from their surgery, but risks do increase with age, and for those with heart, chest or other medical conditions, such as diabetes, obesity, or if you smoke. Risks include:
Chest infection:
To try and prevent this it is important you practice deep breathing, as explained below. Stopping smoking as long as possible before your operation will also help.
Wound infection:
If you notice redness, swelling, discharge from your wounds, tell your nurse, or contact your GP if you have gone home.
Thrombosis (blood clot):
Surgery carries a risk of a clot forming in the leg (this can also happen in the lung). To reduce this risk, a small injection to thin the blood will be given every day. You will also be given some stockings to wear while in hospital, and at home until fully mobile. Regularly exercising your legs, and getting out of bed and walking as much as possible will help reduce problems.
Procedure specific risks
Recurrence
Occasionally recurrence occurs in those who have had an external prolapse prior to surgery, but this is less than 2%. Rarely people with prior ODS experience no symptom improvement following surgery though most experience a significant improvement, as do those with incontinence.
Conversion to open surgery
Occasionally, if you have had extensive abdominal surgery, you may not be suitable for laparoscopic surgery.
Hernia
Occasionally you may develop a bulge or hernia around one of the wounds; you may need a small operation to correct this.
Mesh erosion
Very rarely the mesh may erode though the bowel wall or vagina, this can happen months or even years following surgery. If this occurs you may need surgery to correct this
Recovery from your Operation
It is important that you play an active part in your recovery. The aim is to optimise your recovery process and get you better quicker by reducing some of the risks of complications; ie.
- Earlier mobilisation to prevent blood clots, chest infections etc. Sitting out of bed, and regular walks.
- Eat and drink as soon as you feel like it.
- Good pain relief
Day of Operation (Day 0)
- You will wake up in Recovery, with an oxygen mask. Your blood pressure, pulse and oxygen levels will be monitored. You may sit up as soon as you are awake, and the nurses will make sure you have pain killers and anti sickness medicine as you need. You may have something to drink as soon as you like. When you are comfortable and stable you will be taken back to your ward.
- You will have an intravenous drip, so that you do not become dehydrated, which will be taken out when you are drinking well. There will be a catheter in your bladder so that your urine can be measured.
- If you feel like it you may have something to light to eat on the ward. You will be able to sit out of bed in a chair for a couple of hours later in the day.
- You need to do breathing exercises – breathe in deeply through your nose, and out through your mouth, 5 times, every hour.
- Exercise your calf muscles every hour by stretching and bending your legs, and rotating your ankles.
Day 1 - the first day after your operation.
- You will continue to have pain killers and anti sickness medicine as you require. Make sure the nurse looking after you knows if you have pain.
- Your catheter will be taken out
- You may eat a light diet of whatever you feel like, which you can gradually increase. Eat your meals sitting out of bed
- Continue deep breathing and leg exercises, and walk about as much as you can.
You will probably only need to stay in hospital a night or two. You may not have your bowels open before you go home, but you will be given Movicol (laxative) to take on a regular basis. It is very important that you do not get constipated, and strain at all when opening your bowels, so that you do not strain the stitches holding the mesh in place, or cause pain. Movicol will keep the stool very soft.
Your Recovery
DOs
- Do get up and about both during your hospital stay and after going home.
- Do take regular laxatives (we usually recommend movicol one sachet three times a day) to keep your motions soft.
- Do gradually reduce your laxatives in the six weeks after surgery, if your bowels are too loose. Patients differ enormously in their need for laxatives but it is important that for six weeks, your bowels are on the loose side of normal.
- Do take exercise in the form of walking and swimming as soon as comfortable.
- Do drink plenty of fluids after surgery.
- Do expect that your bowel function will be different after surgery compared to before.
DON’Ts
- Don’t lift anything heavier that a kettle for six weeks after surgery.
- Don’t get constipated or strain when on the toilet.
- Don’t ignore the urge to go to the toilet.
- Don’t be concerned if you do not open your bowel for 4-5 days after surgery. This is quite normal.
- Don’t do running or gym work for six weeks after the surgery.
- Don’t have sexual intercourse for four weeks after the surgery.
- Don’t drive for two weeks after surgery.
- Don’t suffer discomfort unnecessarily. You should take paracetamol regularly if needed. This will not cause constipation.